

Hospital waiting room scenes are dangerous.
Not because they are hard to make emotional. Because they are easy to make emotional in the most obvious way.
People wait. People cry. Someone paces. Someone prays. Doctor appears. Good news or bad news. Scene over.
You have seen this a hundred times.
And most of the time, it feels like narrative pause instead of narrative pressure.
A powerful waiting room scene is not about waiting. It is about what waiting does to people who cannot act directly on the crisis. Control is stripped. Time slows. Old conflicts surface. New alliances form. Information becomes currency. Minor social gestures become charged because no one can fix the central problem.
That is your dramatic engine.
Here is why that matters: waiting rooms are one of the rare places where urgency and powerlessness coexist in the same frame. If you write that contradiction with precision, the scene can be among the most tense in your script without a single chase or fight.
Why Waiting Room Scenes Feel Flat or Manipulative
Most weak scenes fail for one core reason: they mistake situation for conflict.
The situation is already emotional, so writers assume tension is automatic. It is not. Emotion without objective friction becomes repetitive quickly.
Another common problem is medical melodrama shortcutting. Scene leans on beeping monitors, dramatic doctor entrances, and abrupt news drops without character-specific decision pressure.
Then there is reaction uniformity. Everyone processes anxiety in the same way, often through tears and pleading dialogue. Real groups under stress do not regulate the same way. Some become practical. Some become angry. Some go numb. Some focus on logistics because feelings are unbearable.
Think about it this way: if your waiting room scene can be replaced by "they waited anxiously," it is underwritten.
Tension in waiting-room scenes comes from contested coping, not just bad news anticipation.
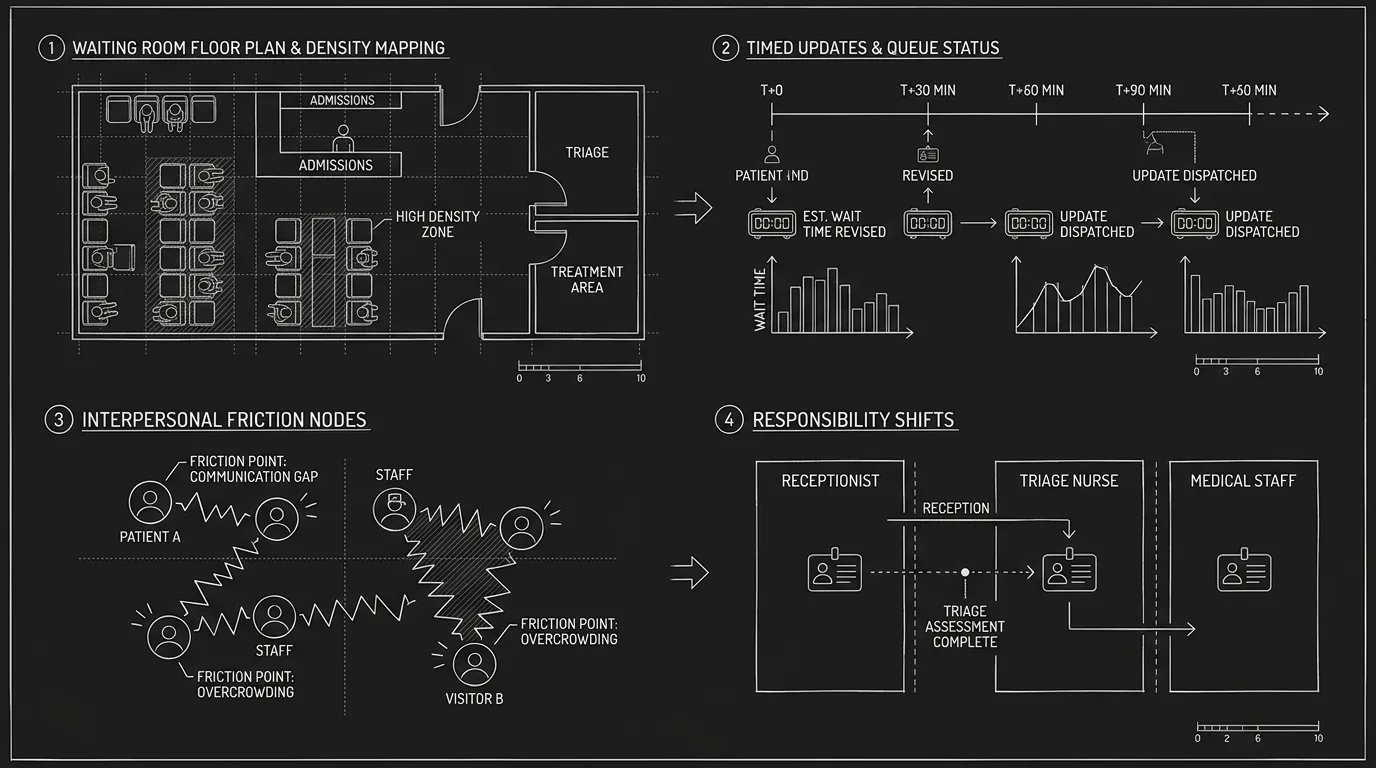
The Core Model: Uncertainty, Constraint, Friction, Update, Reallocation
A high-functioning hospital waiting room scene follows five beats.
Uncertainty: stakes and unknowns are clear.
Constraint: characters cannot directly influence medical event.
Friction: interpersonal agendas clash under stress.
Update: partial information changes perceived odds.
Reallocation: group power, trust, or responsibility shifts.
Without Friction, scene is mood.
Without Update, scene stagnates.
Without Reallocation, scene has no consequence.
Scenario One: Family Waiting for Surgery Outcome
Beginner version: family sits silently, occasional crying, doctor arrives at end with update.
It can feel sincere.
It often lacks progression.
A stronger version gives each family member a competing objective.
One wants optimistic narrative control.
One wants full truth and data.
One wants to hide legal/financial complication.
One wants to call someone the rest refuse to involve.
Now every update creates strategic conflict, not just emotional reaction.
Scenario Two: Waiting Room in a Crime Thriller
In thrillers, waiting rooms are often used as neutral pause before next plot beat.
Missed opportunity.
A better approach treats the waiting room as temporary command vacuum.
Characters are physically contained, under surveillance risk, and vulnerable to information manipulation. A witness can disappear, a phone can be compromised, a false update can reroute key decision-makers.
The medical crisis remains real, but thriller mechanics stay active.
Scenario Three: Waiting Room Scene After Public Incident
When injury follows a public scandal, waiting room scenes can carry reputation pressure alongside fear.
Who can enter?
Who gets blocked?
Who leaks status updates?
Who speaks to press?
Who controls narrative when facts are incomplete?
This dual-pressure design creates rich dramatic texture beyond "will they survive?"
Step-by-Step Workflow for Writing Waiting Room Tension
Step 1: Define Central Unknown and Decision Deadlines
What is unknown?
survival,
neurological outcome,
surgical viability,
legal consent authority.
Then set decision deadlines linked to this unknown.
Deadlines prevent static emotional looping.
Step 2: Assign Coping Style and Agenda to Each Key Character
No two major characters should regulate stress identically.
Give each one:
coping style,
private fear,
immediate objective.
This creates authentic variation and scene movement.
Step 3: Build Waiting Room Geography as Pressure Tool
Hospitals have zones:
chairs,
hallway thresholds,
coffee machine corner,
nurse desk boundary,
bathroom mirror retreat.
Use location shifts to stage escalating micro-conflicts and temporary alliances.
Step 4: Introduce Information in Controlled Increments
Do not drop one giant update only at end.
Use partial updates:
procedure delay,
blood shortage,
consent signature issue,
unexpected specialist request.
Each update should force choice or conflict.
Step 5: Write Practical Tasks as Emotional Catalysts
Forms, calls, insurance, emergency contacts, medication lists, custody permissions. These tasks seem procedural but can expose family fractures and hidden truths fast.
Practicality is not anti-emotion. It is emotion under pressure.
Step 6: Add One External Pressure Vector
Phone from estranged relative.
Law enforcement inquiry.
Media request.
Employer ultimatum.
Caregiver emergency at home.
External vectors prevent hermetic scene drift.
Step 7: End with Responsibility Reallocation
Who stays overnight?
Who signs consent?
Who tells the children?
Who calls the lawyer?
Who is excluded from decisions?
This reallocation gives scene forward force.
Table: Passive Waiting Room Scene vs Tension-Driven Waiting Room Scene
| Dimension | Passive Version | Tension-Driven Version |
|---|---|---|
| Emotional mode | Uniform anxiety | Distinct coping conflicts |
| Information flow | One final doctor update | Incremental, decision-forcing updates |
| Character agency | Mostly reactive | Constrained but strategic actions |
| Setting use | Generic chairs and pacing | Zone-based pressure and movement |
| Stakes | Survival only | Survival plus relational/legal/social consequences |
| Ending | Emotional beat only | Responsibility and power shift |
The Trench Warfare Section: What Beginners Get Wrong (and How to Fix It)
This is the fix list that saves these scenes.
Mistake one: everyone just waits.
Fix by giving each major character a task-linked objective.
Mistake two: same emotional expression for all.
Fix with differentiated coping styles and reaction tempos.
Mistake three: one big update at end only.
Fix with partial updates that force intermediate choices.
Mistake four: no conflict because "this is not the time."
Fix by writing conflict as unavoidable under pressure, even when suppressed.
Mistake five: over-reliance on crying dialogue.
Fix with behavioral tension and compressed lines.
Mistake six: generic hospital atmosphere writing.
Fix with selective sensory specifics that affect decisions.
Mistake seven: no practical stakes.
Fix by adding consent, paperwork, money, or communication constraints.
Mistake eight: doctor as exposition machine.
Fix by keeping medical updates concise and character-centered.
Mistake nine: no history activation.
Fix by letting old fractures surface through present tasks.
Mistake ten: scene exists only to deliver bad news.
Fix by making waiting-room interactions alter relationship dynamics.
Mistake eleven: no witness economy.
Fix by tracking who hears which update first and what they do with it.
Mistake twelve: no boundary control.
Fix by staging who is allowed in/out and who decides.
Mistake thirteen: pacing monotony.
Fix with pressure waves: calm attempt, disruption, escalation, false relief, re-escalation.
Mistake fourteen: all subplots paused.
Fix by integrating at least one external vector from main plot.
Mistake fifteen: no actionable ending.
Fix by ending on clear role or decision transfer.
Mistake sixteen: implausible medical detail overload.
Fix with high-level accuracy and focus on dramatic relevance.
Mistake seventeen: emotional speeches under peak stress.
Fix by fragmenting language and prioritizing direct needs.
Mistake eighteen: no aftermath continuity.
Fix by carrying waiting-room decisions into following scenes.
Mistake nineteen: scene too long without state change.
Fix by ensuring each page changes odds, relationships, or responsibilities.
Mistake twenty: reducing crisis to sentiment.
Fix by combining humanity with procedural and social realism.
Waiting-room scenes become unforgettable when people who cannot control the outcome still expose exactly who they are under uncertainty.
Body Image: Waiting Room Pressure Grid
Try it free
Try Screenweaver for free on your script
It is free. Import your existing project, get a clearer view of your outline, and regain control of your story structure in minutes.
Start FreePractical 45-Minute Rewrite Drill
Take your waiting-room scene and run this pass.
First ten minutes: define each character's coping style and objective.
Next ten minutes: insert two partial medical/logistical updates.
Next ten minutes: add one practical task conflict (consent, contact, payment, authority).
Next ten minutes: stage one external pressure vector.
Final five minutes: rewrite ending with explicit responsibility reallocation.
This pass usually turns static anxiety scenes into active dramatic engines.
Advanced Calibration: Balancing Medical Realism and Dramatic Clarity
You do not need full clinical transcripts to write believable medical tension. But you do need enough procedural truth to avoid soap-opera shortcuts.
Use targeted realism:
uncertainty language ("we need more imaging"),
time estimates with caveats,
consent chain logic,
care-team handoff realities.
Then keep focus on what your characters do with incomplete information.
Another advanced move is false certainty disruption. One character may cling to optimistic certainty. Another insists on worst-case planning. When new data undermines both narratives, power shifts again.
For external script-study reference, the Writers Guild Foundation Library is useful and should be treated as nofollow in publishing workflows.
As discussed in our guide on [how to write a character death scene without melodrama], consequence design matters more than emotional volume.
If waiting-room conflict is social and coded, the framework in [how to write a dinner party scene with hidden conflict] helps stage civility under pressure.
And when crisis updates trigger direct confrontation, the principles in [how to write a final confrontation scene that feels earned] help structure escalation.
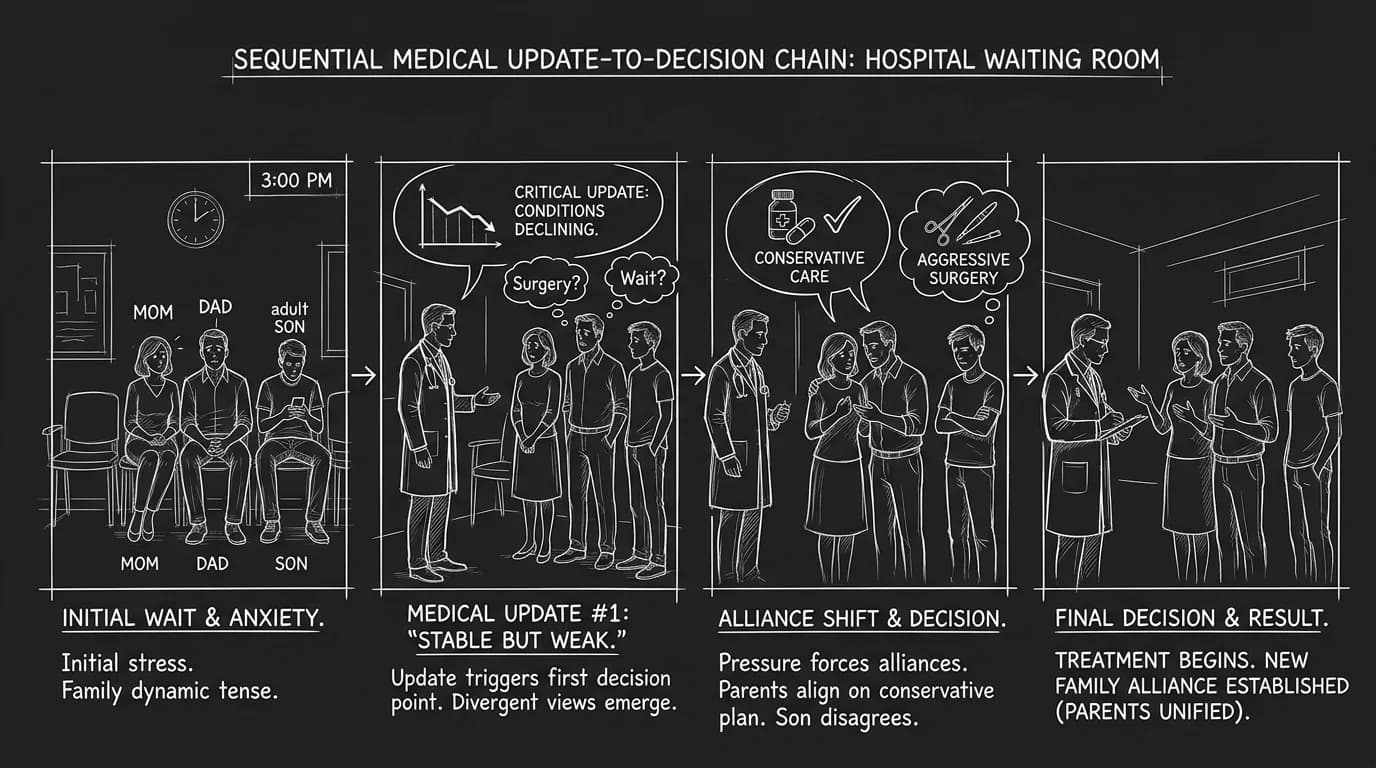
Body Image: Update-to-Decision Chain
YouTube Placeholder
[YOUTUBE VIDEO: A rewrite walkthrough transforming a passive hospital waiting room scene into a high-tension sequence with incremental updates, conflict, and decisive fallout.]
Extra Deep Dive: Writing Time Distortion Without Losing Scene Momentum
Waiting rooms alter time perception.
Five minutes can feel like an hour. An hour can disappear in administrative tasks. Writers often represent this by slowing everything down, but too much slowdown drains narrative energy.
A better approach is controlled temporal contrast.
Alternate between:
compressed practical beats (forms, calls, updates),
and expanded subjective beats (silence, anticipation, cognitive spirals).
This creates emotional realism while preserving momentum.
One useful structure is timestamp anchoring.
You do not need explicit clock stamps every beat, but occasional time markers can sharpen urgency:
"surgery started 47 minutes ago,"
"consultant promised update in ten,"
"ICU transfer decision in thirty."
These anchors convert vague dread into tactical pressure.
Scenario Layer: The Missing Decision-Maker
A high-tension waiting-room variant involves absent authority.
The person legally empowered to sign cannot be reached.
Now scene conflict is procedural and emotional:
who calls whom,
who reveals family fractures,
who lies about authority,
who chooses to proceed anyway.
This kind of pressure avoids melodrama because stakes are specific and immediate.
Writing Institutional Friction
Hospitals are systems, not neutral backdrops. Institutional friction can generate drama without villainizing staff.
Examples:
shift change delays communication,
security access rules block entry,
privacy rules limit updates,
insurance status affects options.
Use institutional constraints as dramatic context, not cynical caricature.
Micro-Exercise: Convert One Emotional Speech into Three Actions
Take one long emotional speech in your draft.
Replace it with:
one short line,
one practical action,
one reaction beat from another character.
This often increases impact because conflict becomes embodied and relational.
Designing Post-Update Silence
After major updates, many writers rush dialogue.
Strategic silence can be stronger.
But silence must be legible. Use one anchor behavior:
someone sits for first time,
someone keeps standing unnaturally still,
someone opens a message thread and closes it unread,
someone removes ring/watch/lanyard unconsciously.
These behaviors turn silence into meaning.
Carrying Waiting-Room Tension into Next Scene
The waiting room should not be an emotional cul-de-sac.
Use one bridge action to transfer pressure:
new caregiver role assigned,
financial decision initiated,
sibling alliance broken,
critical information withheld,
hospital discharge plan disputed.
This bridge ensures the scene has structural consequence, not just atmospheric weight.
Extended Craft Layer: Multi-Family Waiting Rooms and Shared Stress Ecology
Most scripts focus on one family unit. Real waiting rooms often contain multiple unrelated groups under simultaneous stress. You can use this shared ecology to deepen realism and tension.
One family may be loud, another silent.
One receives updates quickly, another waits longer.
One has resources and private room access, another does not.
These contrasts can trigger projection, envy, misplaced anger, unexpected solidarity, or moral discomfort.
Used carefully, background groups can mirror or distort your protagonists' coping strategies.
Writing Peripheral Characters Without Losing Focus
Peripheral waiting-room characters should not steal scene center unless plot requires it.
Give them brief, high-impact beats:
a line that reframes fear,
an interaction that exposes privilege gap,
a practical tip that changes options,
a conflict spark that reveals protagonist stress threshold.
Then return focus to your core arc.
Public Information vs Private Information Channels
Hospitals produce different information channels:
formal clinician updates,
front-desk logistics,
family rumor chain,
text-message relay.
Tension spikes when channels contradict each other.
If one character acts on rumor before formal confirmation, you get immediate conflict with credible stakes.
Designing Ethical Tension Without Villain Framing
Avoid lazy scripts where staff become antagonists for convenience.
Ethical tension can arise naturally from constrained systems:
privacy obligations,
triage priorities,
resource scarcity,
documentation requirements.
Characters can still feel abandoned while the system remains complex rather than cartoonishly cruel.
Practical Beat Sequence for High-Tension Waiting Rooms
If you need a reliable sequence template:
Beat 1: uncertain baseline and role assumptions.
Beat 2: first update creates conflicting interpretations.
Beat 3: practical task triggers family hierarchy dispute.
Beat 4: external vector raises stakes outside hospital.
Beat 5: second update narrows choices sharply.
Beat 6: responsibility transfer locks next-scene direction.
This pattern gives tension progression without melodramatic spikes.
Integrating Quiet Hope Without Sentimental Collapse
Not every waiting-room scene must end dark.
You can include cautious hope if it is grounded in uncertainty.
Avoid "everything is fine now" pivots unless story genuinely supports closure.
A better note is conditional hope:
stability, not certainty,
next procedure needed,
long recovery ahead,
new family burden accepted.
That tone preserves dramatic integrity.
Final Integrity Check
Before locking the scene, ask:
Did at least one update force a decision?
Did character roles shift under pressure?
Did waiting-room behavior reveal deeper history?
Did scene outcome alter next-scene objectives?
If yes, your waiting-room scene is functioning as drama, not pause.
Ending Perspective: Waiting Is Not Inaction
If your hospital waiting room scene feels flat, do not add bigger tears first.
Add sharper pressure architecture.
Who needs what.
Who controls what.
Who knows what.
Who decides what.
Then let uncertainty push those vectors against each other.
Done right, a waiting room scene is not dead air between medical beats.
It is a crucible where relationships, power, and future decisions are forged under fluorescent light and incomplete information.
Final Step
Build your next script with Screenweaver
Move from ideas to production-ready pages faster with timeline-native writing and AI-assisted story flow.
Try Screenweaver